












































Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 [17]
Learning culture
Safeguarding
Safe environments
Safe and effective staffing
Consent to care and treatment
Kindness, compassion and dignity
Providing information
Shared direction and culture
Governance, management and sustainability
Please see the ‘Quality Statements’ section for full guidance
The National Data Opt-Out (https://digital.nhs.uk/services/national-data-opt-out) was introduced on 25 May 2018, to enable NHS patients to opt out from the use of their data for research or planning purposes, in line with the recommendations of the National Data Guardian (NDG).
The national data opt-out implements the opt-out model proposed by the National Data Guardian, as accepted by the Government and directed by the Department of Health and Social Care. The National Data Opt-Out applies to all publically funded health and social care.
This policy and procedure are provided for the regulated activity of personal care.
Our organisation is committed to equal rights and the promotion of choice, person-centred care and independence. This policy demonstrates our commitment to creating a positive culture of respect for all individuals. The intention is, as required by the Equality Act 2010, to identify, remove or minimise discriminatory practice in the nine named protected characteristics of age, disability, sex, gender reassignment, pregnancy and maternity, race, sexual orientation, religion or belief, and marriage and civil partnership. It is also intended to reflect the Human Rights Act 1998 to promote positive practice and value the diversity of all individuals.
1. The National Data Opt-Out was introduced on 25th May 2018, and the deadline for compliance was the 31st July 2022.
2. The national data opt-out implements the opt-out model proposed by the National Data Guardian, as accepted by the Government and directed by the Department of Health and Social Care.
3. The organisation will comply with the Data Protection Act 2018 and General Data Protection Regulations (UK GDPR), including Article 5 – Principles and Article 6 – Lawful Bases for Processing Data, for both public and privately funded delivery of the regulated activity.
4. It is this organisation’s aim to support service users in exercising their right to opt out and to ensure that their data is managed securely in line with all relevant guidance, legislation and regulation including:
5. Data Protection Act 2018 (DPA 2018)
6. UK General Data Protection Regulations (UK GDPR)
7. Code of practice on confidential information, NHS Digital
8.The Seven Caldicott Principles
9. Human Rights Act 1998
10. Common Law Requirement on Confidentiality (CLDC)
This is not an exclusive list and is provided for information and example.
It is the organisation’s aim to support service users in exercising their right to opt out and to ensure that their data is managed securely in line with all relevant guidance, legislation and regulations.
The organisation will comply with the Data Protection Act 2018 and General Data Protection Regulations (UK GDPR), including Article 5 – Principles and Article 6 – Lawful Bases for Processing Data, for both public and privately funded delivery of the regulated activity, i.e:
1. Consent: the individual has given clear consent for the organisation to process their personal data for a specific purpose.
2. Contract: the processing is necessary for a contract you have with the individual, or because they have asked you to take specific steps before entering into a contract.
3. Legal obligation: the processing is necessary for you to comply with the law (not including contractual obligations).
4. Vital interests: the processing is necessary to protect someone’s life.
5. Public task: the processing is necessary for you to perform a task in the public interest or for your official functions, and the task or function has a clear basis in law.
6.Legitimate interests: the processing is necessary for your legitimate interests or the legitimate interests of a third party, unless there is a good reason to protect the individual’s personal data which overrides those legitimate interests. (This cannot apply if you are a public authority processing data to perform your official tasks.)
The organisation will undertake a Data Protection Impact Assessment for each type and category of data being processed to ensure appropriate risk assessments and data management mitigation is in place.
It is our aim to support service users in exercising their right to opt out and to ensure that their data is managed securely in line with all relevant guidance, legislation and regulation including:
i. Data Protection Act 2018 (DPA 2018)
ii. UK General Data Protection Regulations (UK GDPR)
iii. Code of practice on confidential information, NHS Digital
iv. The Seven Caldicott Principles
v. Human Rights Act 1998
vi. Common Law Requirement on Confidentiality (CLDC)
This is not an exclusive list and is provided for information and example.
This is defined by the National Health Service Act 2006 (Section 251B) as information that meets all of the following three requirements:
1. Identifiable or likely identifiable (for example from other data likely to be in the possession of the data recipient), and
2. Given in circumstances where the individual is owed an obligation of confidence, and
3. Conveys some information about the physical or mental health or condition of an individual, a diagnosis of their condition; and/or their care or treatment.
It is important to note that this has been updated to ensure that the definitions used include local authority social care.
The term CPI includes special categories of personal data under Article 9 UK GDPR and also covers information about the deceased as the UK GDPR only applies to living individuals.
The following definition of individual (also called direct) care as set out in the National Data Guardian (NDG) Review is used to underpin the national data opt-out:
‘A clinical, social or public health activity concerned with the prevention, investigation and treatment of illness and the alleviation of suffering of individuals. It includes supporting individuals’ ability to function and improve their participation in life and society.
It includes the assurance of safe and high-quality care and treatment through local audit, the management of untoward or adverse incidents, person satisfaction including measurement of outcomes undertaken by one or more registered and regulated health or social care professionals and their team with whom the individual has a legitimate relationship for their care.’
The NDG review gave some further clarity on local clinical audit as follows:
‘The use of personal confidential data for local clinical audit is permissible within an organisation with the participation of a health and social care professional with a legitimate relationship to the patient through implied consent.
For audit across organisations, the use of personal confidential data is permissible where there is approval under Regulation 5 of the Health Service (Control of Patient Information) Regulations 2002.’
Section 251B and implied consent under CLDC will together provide the lawful basis to share in most cases of direct care. In these cases, and any cases of direct care based on explicit consent, the national data opt-out will not apply.
Indirect care includes:
1. Reviewing the care provided to ensure it is of the highest standard and quality.
2. Ensuring services meet patient needs in the future.
3. Investigating patient queries, complaints and legal claims.
4. Ensuring the hospital receives payment for the care received.
5. Preparing statistics on NHS performance.
6. Auditing NHS accounts and services.
7. Undertaking health research and development (with service users’ consent – you may choose whether or not to be involved).
8. Helping to train and educate healthcare professionals.
Nationally there are strict controls on how patient and service user information is used for these purposes. These decide whether information has to be de-identified first and with whom identifiable information can be shared.
The national data opt-out is a policy to be considered and applied with data protection legislation, other laws and best practice, including data protection legislation and the Common Law Duty of Confidentiality (CLDC), Human Rights Act 1998, and all relevant Codes of Practice of confidentiality and best practice guidance, e.g. the seven Caldicott Principles.
Data protection legislation requires the lawful basis for any processing to be communicated clearly to individuals through appropriate methods and materials in line with the duty of transparency.
The organisation will only manage and use a service user’s personal identifiable data for a lawful purpose, e.g:
1. For individual or direct care OR
2. Sharing with other health or social care providers providing care to the service user
In either case the opt-out does not apply.
Any other purpose beyond individual care will be assessed on a case-by-case basis, and data will be provided in an anonymised form where there is a contractual or legal requirement to provide the information where it does not directly pertain to the delivery of care.
The national data opt-out does not apply to information that is anonymised in line with the Information Commissioner’s Office (ICO) Code of Practice (CoP) on Anonymisation or is aggregate or count type data.
It does not apply to workforce or staff information, which is subject to UK GDPR and DPA 2018 protections.
A number of different channels are available for the public to set a national data opt-out. These are:
1. A digital (online) channel accessed via the national data opt-out service. National Data Opt-Out, NHS Digital (https://digital.nhs.uk/services/national-data-opt-out)
2. For those who need support to set their national data opt-out preference online a digitally- assisted channel is provided that enables members of the public to set a national data opt-out with assistance from NHS Digital staff via the national helpline.
3. NHS Digital Contact Centre phone number: 0300 303 5678 – Monday to Friday, 9am to 5pm (excluding bank holidays).
4. A non-digital (paper based) channel accessed by the national helpline or through forms which can be printed from the webpages
5. If they are a parent or legal guardian and they want to opt their children out, they must complete the opt-out form. Manage your choice, or your child’s choice on their behalf (https://assets.nhs.uk/prod/documents/Manage_your_childs_choice_on_their_behalf.pdf)
6. Once they have completed the form, they can email it to the Contact Centre at [email protected] (mailto:[email protected]) or via the NHS App (https://www.nhs.uk/nhs-services/online-services/nhs-app/)
There are some points that apply to specific groups with respect to setting a national data opt-out:
i. Individuals aged 13 or over are able to set a national data opt-out via the digital, digitally-assisted and non-digital channels.
ii. Those with parental responsibility (parents and legal guardians), are able to set a national data opt-out on behalf of a child under the age of 13 via the non-digital channel only.
iii. There is a specific form that allows a choice to be set for up to six children at once.
iv. Any national data opt-out that has been set by a person with parental responsibility for a child under the age of 13 will remain in place unless and until it is proactively changed.
v. Those who have a formal proxy relationship to make decisions on behalf of another adult (either a lasting power of attorney or a court appointed deputy) are able to set a national data opt-out on behalf of that person via the non-digital channel only.
vi. Individuals in the secure and detained estate (e.g. prisons) are able to set a national data opt-out through the healthcare professionals working in these settings.
vii. Individuals who have agreed with their GP for their records to be marked as sensitive will be offered the choice to set a national data opt-out through the established processes to set (or remove) a sensitive flag.
viii. A national data opt-out cannot be set for a deceased patient unless they have explicitly stated this in a last will or testament. This can only be done via the non-digital channel.
A national data opt-out is stored against a person’s individual record on the NHS Digital Spine against their NHS number.
Any person registered with an NHS number allocated to them is able to set a national data opt-out. This covers the majority of patients and service users who have received health or care services in England and, therefore, have data about them in the health and care system in England.
A child is able to set their own opt-out from age 13 which aligns with the minimum age at which children can give their consent to participate in digital services as set out in data protection legislation.
This is not based on any test of competence. Children under 13 and those who lack capacity are not able to set an opt-out themselves. In these cases, individuals who have a formal, legal relationship to act on behalf of them (i.e. somebody who has parental responsibility, a lasting power of attorney or court appointed deputy) are able to set an opt-out on their behalf by proxy.
The national data opt-out is defined based on purpose and applies to any disclosure of data for purposes other than individual or direct care.
Purposes other than individual care or direct care are defined as anything that does not meet the definition of individual care or direct care.
See ‘National Data opt-out, Appendix 2: Definitions (https://digital.nhs.uk/services/national-data-opt-out/operational-policy-guidance-document/appendix-2-definitions).’
It would include purposes such as planning for the provision of:
1. Local services
2. Managing and running NHS and adult social care services
3. Commissioning
4. Invoice validation
5. National clinical audits and research
The national data opt-out applies to data relating to publicly funded or arranged care only, i.e. by a local authority, ICB or NHS commissioner. This includes where the care is provided by a private provider and the service is fully or partially funded by the public body.
This is summarised as:
• All NHS organisations (including private patients treated within such organisations).
• Adult social care which is funded or arranged by a public body (typically a local authority).
• NHS arranged care within private providers (e.g. Nuffield, BMI Healthcare).
• Any release of data by NHS Digital which relates to private patients including that which is collected by a request under S259 of the Health and Social Care Act 2012 (HSCA).
• Privately (non-NHS) funded patients within private providers unless the care is funded or arranged by a public body.
• Care which is not provided or arranged by a public body, that is privately arranged/privately funded care.
It is of note that in adult social care, providers typically have a range of patients receiving both publicly funded and privately funded care in the same care service. The funding arrangements for individual service users may also change several times over short time periods. Under these circumstances:
• The organisation will review the best position for service users and may extend the national data opt-out to cover all the service users in order to make implementation within the service straightforward.
• In the case a voluntary extension is implemented, the organisation will make clear to services users, via contracts for the provision of care, privacy notices, and other provided information, the opportunity to opt out and the process.
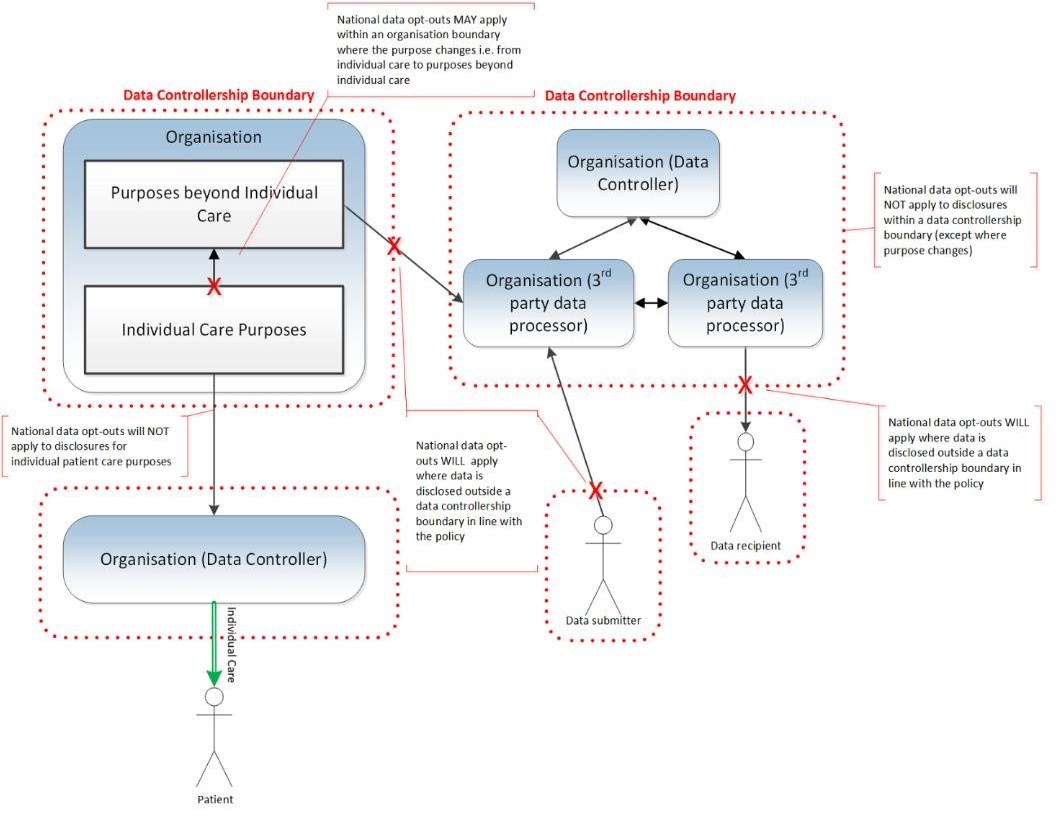
Data controllers, whether solely or jointly with another organisation, are responsible for ensuring that national data opt-outs are applied in line with the ‘National Data Opt-Out Policy.’
In some cases this will require data controllers to instruct any organisations acting as a data processors under their instruction to apply the national data opt-out.
For our organisation it is most likely that the local authority, ICB or NHS commissioners who act as the data controllers will notify the service of the opt-out of the service user. The organisation, as the data processor, will then register within the services user’s care records the opt-out and comply with the notification related to sharing for the purposes of Indirect Care, including data for research or planning purposes.
Data controllers must apply national data opt-outs whenever confidential patient information is to be disclosed outside of their data controllership boundary in line with the wider policy (see ‘figure 1’ below) and is relying on section 251 support. Data controllers may also need to apply national data opt-outs for internal uses of the data where the purpose changes from individual care and the disclosure is relying on S.251 support to be lawful.
Further information on the responsibilities of data controllers is provided by the ICO (https://ico.org.uk/for-organisations/uk-gdpr-guidance-and-resources/controllers-and-processors/).
(https://www.igt.hscic.gov.uk/Resources/Data%20Controllers%20for%20shared%20records%20.pdf)
does the opt-out apply to? For the original diagram please see ‘Which organisation (https://digital.nhs.uk/services/national-data-opt-out/operational-policy-guidance-document/which-organisations-does-the-opt-out-apply-to)’
National data opt-out, NHS Digital (https://digital.nhs.uk/services/national-data-opt-out/national-data-opt-out-new)
Overview: Choose if data from your health records is shared for research and planning, NHS (https://www.nhs.uk/your-nhs-data-matters/)
National data opt-out, Digital SocialCare (https://www.digitalsocialcare.co.uk/national-dataoptout/#:~:text=Under%20the%20national%20data%20opt,or%20delivering%20their%20own%20care)
National Data opt-out; Appendix 2: Definitions, NHS Digital (https://digital.nhs.uk/services/national-data-opt-out/operational-policy-guidance-document/appendix-2-definitions)
Manage your choice, or your child’s choice on their behalf, NHS
(https://assets.nhs.uk/prod/documents/Manage_your_childs_choice_on_their_behalf.pdf)
Quality Statements
We have a proactive and positive culture of safety based on openness and honesty, in which concerns about safety are listened to, safety events are investigated and reported thoroughly, and lessons are learned to continually identify and embed good practices.
We work with people to understand what being safe means to them as well as with our partners on the best way to achieve this. We concentrate on improving people’s lives while protecting their right to live in safety, free from bullying, harassment, abuse, discrimination, avoidable harm and neglect. We make sure we share concerns quickly and appropriately.
We detect and control potential risks in the care environment. We make sure that the equipment, facilities and technology support the delivery of safe care.
We make sure there are enough qualified, skilled and experienced people, who receive effective support, supervision and development. They work together effectively to provide safe care that meets people’s individual needs.
We tell people about their rights around consent and respect these when we deliver person-centred care and treatment.
We always treat people with kindness, empathy and compassion and we respect their privacy and dignity. We treat colleagues from other organisations with kindness and respect.
We treat people as individuals and make sure their care, support and treatment meets their needs and preferences. We take account of their strengths, abilities, aspirations, culture and unique backgrounds and protected characteristics.
We promote people’s independence, so they know their rights and have choice and control over their own care, treatment and well-being.
We make sure people are at the centre of their care and treatment choices and we decide, in partnership with them, how to respond to any relevant changes in their needs.
We provide appropriate, accurate and up-to-date information in formats that we tailor to individual needs.
We have a shared vision, strategy and culture. This is based on transparency, equity, equality and human rights, diversity and inclusion, engagement, and understanding challenges and the needs of people and our communities in order to meet these.
We have clear responsibilities, roles, systems of accountability and good governance. We use these to manage and deliver good quality, sustainable care, treatment and support. We act on the best information about risk, performance and outcomes, and we share this securely with others when appropriate.
Key questions and quality statements – Care Quality Commission (https://www.cqc.org.uk/assessment/quality-statements)